


References
- Pap R, van Loggerenberg C. A comparison of airway management devices in simulated entrapment-trauma: a prospective manikin study. Int J Emerg Med. 2019 Jul 8;12(1):15. doi: 10.1186/s12245-019-0233-z. PMID: 31286862; PMCID: PMC6615147.
- Kornhall D, Hellikson F, Näslund R, Lind F, Broms J, Gellerfors M. A Protocol for Helicopter In-Cabin Intubation. Air Med J. 2018 Sep;37(5):306-311. doi: 10.1016/j.amj.2018.05.002. Epub 2018 Jun 7. PMID: 30322633.
- Koetter KP, Hilker T, Genzwuerker HV, Lenz M, Maleck WH, Petroianu GA, Fisher JA. A randomized comparison of rescuer positions for intubation on the ground. Prehosp Emerg Care. 1997 Apr-Jun;1(2):96-9. doi: 10.1080/10903129708958796. PMID: 9709346.
- Nakstad AR, Sandberg M. Airway management in simulated restricted access to a patient--can manikin-based studies provide relevant data? Scand J Trauma Resusc Emerg Med. 2011 Jun 13;19:36. doi: 10.1186/1757-7241-19-36. PMID: 21668944; PMCID: PMC3125355.
- McCaul CL, Harney D, Ryan M, Moran C, Kavanagh BP, Boylan JF. Airway management in the lateral position: a randomized controlled trial. Anesth Analg. 2005 Oct;101(4):1221-1225. doi: 10.1213/01.ane.0000171712.44746.bb. PMID: 16192549.
- Lim JA, Jeong MY, Kim JH. Airway management using laryngeal mask airway (LMA) in a patient in a lateral decubitus position: A case report. Medicine (Baltimore). 2019 Dec;98(51):e18287. doi: 10.1097/MD.0000000000018287. PMID: 31860976; PMCID: PMC6940134.
- Komatsu R, Kamata K, You J, Sessler DI, Kasuya Y. Airway scope for tracheal intubation in the lateral position. Anesth Analg. 2011 Apr;112(4):868-74. doi: 10.1213/ANE.0b013e31820c7cdf. Epub 2011 Mar 8. PMID: 21385975.
- Zhang J, Lamb A, Hung O, Hung C, Hung D. Blind nasal intubation: teaching a dying art. Can J Anaesth. 2014 Nov;61(11):1055-6. doi: 10.1007/s12630-014-0223-9. Epub 2014 Aug 15. PMID: 25125251.
- Thomas SH, Farkas A, Wedel SK. Cabin configuration and prolonged oral endotracheal intubation in the AS365N2 Dauphin EMS helicopter. Air Med J. 1996 Apr-Jun;15(2):65-8. doi: 10.1016/s1067-991x(96)90003-6. PMID: 10158162.
- Matthew Deibel and David T. Lock and Jeffrey Jones and John D Hoyle and M. Bernadotte. Comparative Study of Airway Management During Confined-Space Urban Rescue}. Annals of Emergency Medicine, 2005, vol 46; pages 4-5.
- Hoyle JD Jr, Jones JS, Deibel M, Lock DT, Reischman D. Comparative study of airway management techniques with restricted access to patient airway. Prehosp Emerg Care. 2007 Jul-Sep;11(3):330-6. doi: 10.1080/10903120701205083. PMID: 17613909.
- Martin AB, Lingg J, Lubin JS. Comparison of Airway Management Methods in Entrapped Patients: A Manikin Study.Prehosp Emerg Care. 2016 Sep-Oct;20(5):657-61. doi: 10.3109/10903127.2016.1139218. Epub 2016 Mar 8. PMID: 26954013.
- Steinmann D, Ahne T, Heringhaus C, Goebel U. Comparison of airway management techniques for different access in a simulated motor vehicle entrapment scenario. Eur J Emerg Med. 2016 Aug;23(4):279-285. doi: 10.1097/MEJ.0000000000000254. PMID: 25715022.
- Genzwürker, Harald, Krahl, S., Finteis, F., Hinkelbein, Jochen. Comparison of different strategies for ventilation in a simulation of an entrapped car accident victim. EUR J ANAESTH. 2007/06/01. Vol 24. Doi: 10.1097/00003643-200706001-00609.
- Truszewski Z, Szarpak Ł, Smereka J, Kurowski A, Evrin T, Czyzewski Ł. Comparison of the VivaSight single lumen endotracheal tube and the Macintosh laryngoscope for emergency intubation by experienced paramedics in a standardized airway manikin with restricted access: a randomized, crossover trial. Am J Emerg Med. 2016 May;34(5):929-30. doi: 10.1016/j.ajem.2016.02.054. Epub 2016 Feb 27. PMID: 26979260.
- Wang Y, Shi Y, Li YX, Zhong M, Zhuang YR, Huang W, Ma WH. Comparison of tracheal intubation between sitting position and standing position in COVID-19 patients: A manikin study. Medicine (Baltimore). 2021 Nov 5;100(44):e27529. doi: 10.1097/MD.0000000000027529. PMID: 34871215; PMCID: PMC8568451.
- Kaminska H, Wieczorek W. Comparison of two types of laryngoscopy for face-to-face intubation of a patient entrapped in a vehicle. Am J Emerg Med. 2018 Oct;36(10):1898-1899. doi: 10.1016/j.ajem.2018.01.099. Epub 2018 Jan 31. PMID: 29429795.
- Hulme J, Perkins GD. Critically injured patients, inaccessible airways, and laryngeal mask airways. Emerg Med J. 2005 Oct;22(10):742-4. doi: 10.1136/emj.2005.026443. PMID: 16189045; PMCID: PMC1726560.
- Adnet F, Cydulka RK, Lapandry C. Emergency tracheal intubation of patients lying supine on the ground: influence of operator body position. Can J Anaesth. 1998 Mar;45(3):266-9. doi: 10.1007/BF03012914. PMID: 9579267.
- Givens GC, Shelton SL, Brown EA. Emergency cricothyrotomy in confined space airway emergencies: a comparison. Prehosp Disaster Med. 2011 Aug;26(4):259-61. doi: 10.1017/S1049023X11006352. PMID: 21996279.
- Helm M, Hossfeld B, Schäfer S, Hoitz J, Lampl L. Factors influencing emergency intubation in the pre-hospital setting--a multicentre study in the German Helicopter Emergency Medical Service. Br J Anaesth. 2006 Jan;96(1):67-71. doi: 10.1093/bja/aei275. Epub 2005 Nov 25. PMID: 16311285.
- Thomas SH, Harrison T, Wedel SK. Flight crew airway management in four settings: a six-year review. Prehosp Emerg Care. 1999 Oct-Dec;3(4):310-5. doi: 10.1080/10903129908958960. PMID: 10534031.
- Harrison T, Thomas SH, Wedel SK. In-flight oral endotracheal intubation. Am J Emerg Med. 1997 Oct;15(6):558-61. doi: 10.1016/s0735-6757(97)90156-x. PMID: 9337360.
- Gaszynska E, Samsel P, Stankiewicz-Rudnicki M, Wieczorek A, Gaszynski T. Intubation by paramedics using the ILMA or AirTraq, KingVision, and Macintosh laryngoscopes in vehicle-entrapped patients: a manikin study. Eur J Emerg Med. 2014 Feb;21(1):61-4. doi: 10.1097/MEJ.0b013e3283632fb6. PMID: 23778270.
- Maeyama H, Naito H, Guyette FX, Yorifuji T, Banshotani Y, Matsui D, Yumoto T, Nakao A, Kobayashi M. Intubation during a medevac flight: safety and effect on total prehospital time in the helicopter emergency medical service system. Scand J Trauma Resusc Emerg Med. 2020 Sep 7;28(1):89. doi: 10.1186/s13049-020-00784-z. PMID: 32894186; PMCID: PMC7487559.
- Hilker T, Genzwuerker HV. Inverse intubation: an important alternative for intubation in the streets. Prehosp Emerg Care. 1999 Jan-Mar;3(1):74-6. doi: 10.1080/10903129908958911. PMID: 9921746.
- Robinson K, Donaghy K, Katz R. Inverse intubation in air medical transport. Air Med J. 2004 Jan-Feb;23(1):40-3. doi: 10.1016/j.amj.2003.10.007. PMID: 14760307.
- Schober P, Krage R, van Groeningen D, Loer SA, Schwarte LA. Inverse intubation in entrapped trauma casualties: a simulator based, randomised cross-over comparison of direct, indirect and video laryngoscopy. Emerg Med J. 2014 Dec;31(12):959-63. doi: 10.1136/emermed-2012-202064. Epub 2013 Sep 4. PMID: 24005641.
- Adnet F, Lapostolle F, Borron SW, Hennequin B, Leclercq G, Fleury M. Optimization of glottic exposure during intubation of a patient lying supine on the ground. Am J Emerg Med. 1997 Oct;15(6):555-7. doi: 10.1016/s0735-6757(97)90155-8. PMID: 9337359.
- Gellerfors M, Fevang E, Bäckman A, Krüger A, Mikkelsen S, Nurmi J, Rognås L, Sandström E, Skallsjö G, Svensén C, Gryth D, Lossius HM. Pre-hospital advanced airway management by anaesthetist and nurse anaesthetist critical care teams: a prospective observational study of 2028 pre-hospital tracheal intubations. Br J Anaesth. 2018 May;120(5):1103-1109. doi: 10.1016/j.bja.2017.12.036. PMID: 29661387.
- Broms J, Linhardt C, Fevang E, Helliksson F, Skallsjö G, Haugland H, Knudsen JS, Bekkevold M, Tvede MF, Brandenstein P, Hansen TM, Krüger A, Rognås L, Lossius HM, Gellerfors M. Prehospital tracheal intubations by anaesthetist-staffed critical care teams: a prospective observational multicentre study. Br J Anaesth. 2023 Dec;131(6):1102-1111. doi: 10.1016/j.bja.2023.09.013. Epub 2023 Oct 14. PMID: 37845108.
- Braude D, Richards M. Rapid Sequence Airway (RSA)--a novel approach to prehospital airway management. Prehosp Emerg Care. 2007 Apr-Jun;11(2):250-2. doi: 10.1080/10903120701206032. PMID: 17454819.
- Braude D, Southard A, Bajema T, Sims E, Martinez J. Rapid sequence airway using the LMA-Supreme as a primary airway for 9 h in a multi-system trauma patient. Resuscitation. 2010 Sep;81(9):1217. doi: 10.1016/j.resuscitation.2010.06.001. Epub 2010 Jul 4. PMID: 20599313.
- Southard A, Braude D, Crandall C. Rapid sequence airway vs rapid sequence intubation in a simulated trauma airway by flight crew. Resuscitation. 2010 May;81(5):576-8. doi: 10.1016/j.resuscitation.2009.12.026. Epub 2010 Feb 18. PMID: 20171002.
- Tesler J, Rucker J, Sommer D, Vesely A, McClusky S, Koetter KP, Maleck WH, Fisher JA, Petroianu GA. Rescuer position for tracheal intubation on the ground. 2003 Jan;56(1):83-9. doi: 10.1016/s0300-9572(02)00293-9. PMID: 12505743.
- Tzong‐Luen Wang and Kuo Chih Chen and Hsueh-Ju Teng and Hang. Role of Laryngeal Mask Airway in First Aids in Confined Space. Ann Disaster Med. Vol. 1, No. 2, 2003
- Amathieu R, Sudrial J, Abdi W, Luis D, Hahouache H, Combes X, Dhonneur G. Simulating face-to-face tracheal intubation of a trapped patient: a randomized comparison of the LMA Fastrach™, the GlideScope™, and the Airtraq™ laryngoscope. Br J Anaesth. 2012 Jan;108(1):140-5. doi: 10.1093/bja/aer327. Epub 2011 Oct 27. PMID: 22037225.
- Wetsch WA, Carlitscheck M, Spelten O, Teschendorf P, Hellmich M, Genzwürker HV, Hinkelbein J. Success rates and endotracheal tube insertion times of experienced emergency physicians using five video laryngoscopes: a randomised trial in a simulated trapped car accident victim. Eur J Anaesthesiol. 2011 Dec;28(12):849-58. doi: 10.1097/EJA.0b013e32834c7c7f. PMID: 21986981.
- Komatsu R, Nagata O, Sessler DI, Ozaki M. The intubating laryngeal mask airway facilitates tracheal intubation in the lateral position. Anesth Analg. 2004 Mar;98(3):858-61, table of contents. doi: 10.1213/01.ane.0000100741.46539.6b. PMID: 14980953; PMCID: PMC1350644.
- Castro-Gómez A, Delgadob LA. Intubacion orotraqueal en prono: otra manera para acceder a la via aerea. Rev Colomb Anestesiol. 2017;45:340–343.
- Asai T. Tracheal intubation with restricted access: a randomised comparison of the Pentax-Airway Scope and Macintosh laryngoscope in a manikin. Anaesthesia. 2009 Oct;64(10):1114-7. doi: 10.1111/j.1365-2044.2009.06014.x. PMID: 19735403.
- Dhonneur G, Zraier S, Sebbah JL, Haouache H. Urgent face-to-face tracheal re-intubation using Video-Airtraq™ in ICU patients placed in the sitting position. Intensive Care Med. 2014 Apr;40(4):625-6. doi: 10.1007/s00134-014-3209-8. Epub 2014 Feb 7. PMID: 24504640.
How do I get to attend the course?
To maintain the extremely high lecturer-to-participant ratio we are forced to limit the number of participants.
Therefore, not all applicants will get the opportunity to attend the course - at least not this time.
In order to continuously improve the course, we appreciate motivation, diverse background and experience.
Diversity is key, so we welcome applications from both novices and experts in airway management.
Here is how to do:
Submit your application as soon as possible
Wait patiently for an answer until April 15th 2024
If your application is accepted, you will receive further instructions (payment instructions, promo code for 20% discount on Core Topics in Airway Management and more).
If your application is NOT accepted in the first round, you will stay on the waiting list for possible later acceptance or receive information about coming courses.
Your place on the course is guaranteed only after you have received a confirmation of payment reception
Infrared flashing light (IRRIS) applied after failed attempts at videolaryngoscopy and failed flexible optical intubation:
Tube Tip In Pharynx (TTIP) – for awake flexible bronchoscope-guided oral intubation in patients with extremely restricted mouth-opening:

Airway lecture topics
Managing the airway in the critically Ill
Maintaining oxygenation throughout airway management
Using infrared light to find the trachea
Intubation via a supraglottic airway while maintaining ventilation
Managing the airway with simple means (Including retrograde intubation and Tube-Tip-In-pharynx ventilation)
Identifying the cricothyroid membrane with ultrasonography
Managing the Bleeding upper airway
Managing the airway in a highly contagious (eg corona-virus infected) patient
Workshop topics
Ultrasound-locating the cricothyroid membrane (Wendy Teoh)
Tube Tip In Pharynx (TTIP) ventilation (Jacob Stensballe)
Retrograde intubation on a larynx model (Michael Friis Tvede)
Mask ventilation reinvented! (Hans van Schuppen)
RED° The Bleeding Airway Man (Søren Rudolph and Michael Kristensen)
How to intubate when you can’t see anything!
Dedicated (”SALAD”) suctioning
Flexible optical intubation via SGA
Retrograde intubation
Blinking Infrared light (IRRIS)
IRRIS Patient # 1 |
| Video from the flexible scope |
|
|
IRRIS Patient # 1 |
| Video from the flexible scope |
|
|
IRRIS Patient # 2 |
| Video from the flexible scope |
|
|
IRRIS Patient # 3 |
| Video from the flexible scope |
|
|
IRRIS Patient # 4 (a) |
| Video from the flexible scope |
|
|
IRRIS Patient #4 (b) |
| IRRIS guided intubation seen from the outside |
|
|
IRRIS Patient # 5 |
| Video from the flexible scope |
|
|
IRRIS Patient # 6 |
| Video from the flexible scope |
|
|
IRRIS Patient # 7 |
| Video from the flexible scope |
|
|
IRRIS Patient # 8 |
| Video from the flexible scope |
|
|
IRRIS Patient # 9 |
| Video from the flexible scope |
|
|
IRRIS Patient # 10 |
| Video from the flexible scope |
|
|
Supplemental table S1 |
IRRIS Patient # 2 |
| Video from the flexible scope |
|
|
IRRIS Patient # 3 |
| Video from the flexible scope |
|
|
IRRIS Patient # 4 (a) |
| Video from the flexible scope |
|
|
IRRIS Patient # 5 |
| Video from the flexible scope |
|
|
IRRIS Patient # 6 |
| Video from the flexible scope |
|
|
IRRIS Patient # 7 |
| Video from the flexible scope |
|
|
IRRIS Patient # 8 |
| Video from the flexible scope |
|
|
IRRIS Patient # 9 |
| Video from the flexible scope |
|
|
IRRIS Patient # 10 |
| Video from the flexible scope |
|
|
IRRIS Patient # 4 (b) |
| IRRIS guided intubation seen from the outside |
|
|
Retrograde intubation |
||||||||||||||||||||||||||
| Bleeding patient | ||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
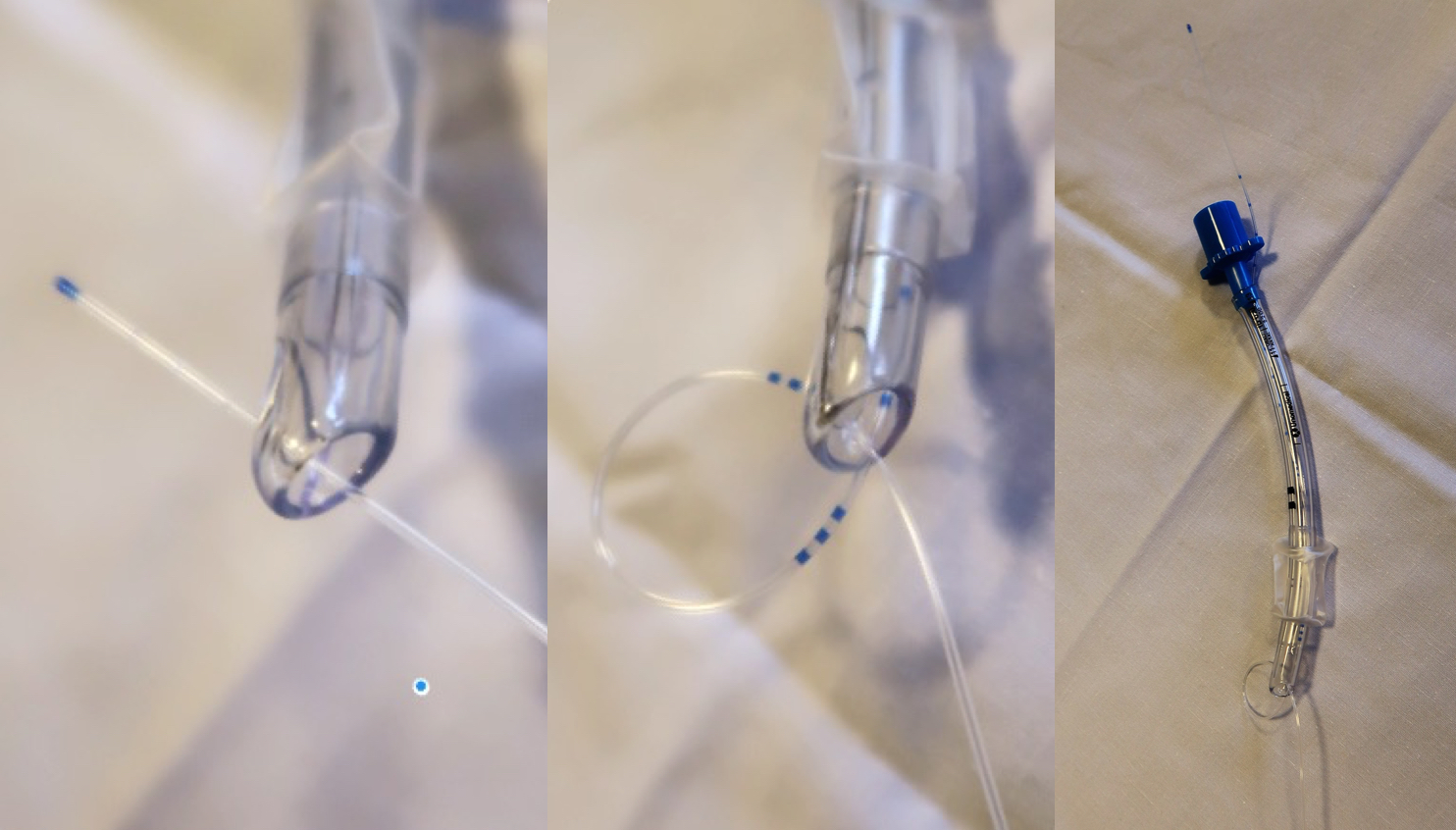
Retrograde intubation with epidural catheter technique intubation |
 |
|
The epidural catheter is lubricated and introduced via the distal end of the tube and out via the Murphy-hole (a) and back into the tube from the distal end (b) and advanced all the way through the tube until it protrudes from the cranial end. The proximal connection of the tube is reinserted so that the epidural catheter is fixed between the tube and the connector (c). Picture courtesy of the Scandinavian airway management course airwaymanagement.dk |
Table. Retrograde intubation in the awake, bleeding and sitting patient: One possible approach. |
|
| Step | |
| 1 | Identification of the cricothyroid membrane with inspection and palpation and/or with ultrasonography |
| 2 | Insertion of an 18 G venous cannula or a Tuohy cannula, through the cricothyroid membrane |
| 3 | Insertion of an epidural catheter via the venous cannula and advanced in a cephalad direction until it exits the mouth (Figure 1) or the patient spits it out or it can be pulled out with a gloved finger or a pair of Magill forceps |
| 4 | The epidural catheter is lubricated and introduced via the distal end of a 5-6 mm internal diameter tube and out via the Murphy eye; back into the tube from the distal end and advanced all the way through the tube until it protrudes from the cranial end. The proximal connection of the tube is then reinserted so that the epidural catheter is fixed between the tube and the connector. Illustration available at: http://airwaymanagement.dk/retrograde/knot. |
| 5 | The catheter is then pulled downwards from the end that protrudes from the cricothyroid membrane, thus pulling down the tracheal tube through the mouth and into the larynx. |
| 6 | When resistance is met, the tip of the tube is at the inside of the cricothyroid membrane and can be pulled no further. |
| 7 | The pulling on the distal part of the catheter is stopped and the tube is pushed distally until it is in the trachea. If the tube impinges on the arytenoid cartilages, it may be gently rotated or a flexible fibrescope may be passed down the tube to visualize passage into the trachea. |
| 8 | The cuff is inflated and the location of the tube in the airway is verified with capnography |
| 9 | The patient can be anaesthetised and haemostasis surgery performed |
| 10 | Extubation can be performed by pulling the tube (having released the catheter from the tube connector) while holding taught on the distal end of the catheter, thus letting the catheter unwind while withdrawing the tube. In this way, the catheter can be left in situ in recovery to potentially provide a guide for re-intubation. |
| Legend to table. A technique for retrograde intubation using readily available equipment, an epidural catheter. The technique described is modified from Abou-Madi 1989. A link to a video of the procedure is here: http://airwaymanagement.dk/retrograde | |
 Dr. Adam Law is Professor of Anaesthesia at the QEII Health Sciences Centre in Halifax, Nova Scotia, Canada. He started medical practice with 6 years as a rural general practitioner. This was followed by a residency in Anaesthesia and subspecialty training in neuroanaesthesia at Western University in London, Ontario, Canada. He has worked in Halifax as a consultant anaesthetist ever since. Adam is co-director of both the US-based Difficult Airway Course and the Canadian AIME airway course and teaches in both courses on a regular basis. He also chaired the Canadian Airway Focus Group, which published expanded and updated Canadian airway management guidelines in 2013. When not at work, he enjoys spending time his family, hiking, running, skiing and playing tennis.
Dr. Adam Law is Professor of Anaesthesia at the QEII Health Sciences Centre in Halifax, Nova Scotia, Canada. He started medical practice with 6 years as a rural general practitioner. This was followed by a residency in Anaesthesia and subspecialty training in neuroanaesthesia at Western University in London, Ontario, Canada. He has worked in Halifax as a consultant anaesthetist ever since. Adam is co-director of both the US-based Difficult Airway Course and the Canadian AIME airway course and teaches in both courses on a regular basis. He also chaired the Canadian Airway Focus Group, which published expanded and updated Canadian airway management guidelines in 2013. When not at work, he enjoys spending time his family, hiking, running, skiing and playing tennis.

Dr. Ana M. López, MD, PhD, DESA is presently a Consultant Anesthetist at the Ambulatory Surgery Unit at Hospital Clinic of Barcelona and Associate Professor of Anesthesiology at the Faculty of Medicine, University of Barcelona. As a board member of the Airway Management Section of the Catalan Society of Anesthesiology (SCARTD), she contributed to the development and update of local guidelines, and is involved in training and continuing education programs in safe airway management. Her research and academic interests are supraglottic airway devices, airway management data analysis, perioperative ultrasound, patient safety and education. She has co-authored several peer-reviewed journal articles and book chapters in these fields.
 |
I’m a Clinical Associate Professor at the University of British Columbia and practice cardiothoracic anaesthesia at Vancouver General Hospital. My teaching and research passions surround multidisciplinary decision-making, shared experiences, and complications associated with airway management. My other roles include being a Royal College of Canada examiner, assistant head of the Canadian Airway Focus group and questioning what we think we know with brilliant airway collaborators. Last year I was awarded the University of British Columbia Faculty of Medicine’s Excellence in Clinical Teaching Award. |
 |
Dr. David Wong is a Professor of Anesthesiology at the University to Toronto. He obtained his MD at University of Toronto in 1981, completed fellowships at University of Toronto and George Washington University, and joined as anesthesia staff at Toronto Western Hospital in 1990. His areas of clinical and research interest include difficult airway management, high flow nasal oxygenation, ultrasound of airway, morbid obesity and surgical airway. Currently, he is the Director of preadmission program, Toronto Western Hospital; Chair of Ambulatory section, Canadian Anesthesiologists’ Society, and Co-Director of the Toronto Anesthesia Symposium. Dr. Wong has published extensively- 138 peer reviewed manuscripts, 10 book chapters and provided over 210 invited lectures. His personal interests include travel, photography, music and NFL football. Currently: Publications: (December 2018) Invited lectures/workshops: 216 Research interests: Education: |
 |
Born and raised between cows and ski slopes, educated at the University of Berne, Switzerland and in various hospitals throughout Switzerland. Always longing for the sight of the ocean, hence stayed in Miami during academic leave. Returned to Switzerland, since then dedicated to airway management. Currently head of department at a regional hospital between Berne and Zurich.
|

 |
Prof. Sheila Nainan Myatra MD, FCCM, FICCM President Elect World Federation of Societies of Anaesthesiologists (WFSA)
Immediate PastPresident
All India Difficult Airway Association (AIDAA) Country Lead (India)
|
The deadline for uploading cases was October 27th, so unfortunately we will have to do without your contribution this time
 |
PD Dr. med. Martin Petzoldt, MD, FEAMS |
FREE DOWNLOAD: The ultimate review on Ultrasonography and airway management
|
Identification of the cricothyroid membrane with ultrasonography |
|
|
FREE DOWNLOAD: The ultimate review on Ultrasonography and airway management
|
Identification of the cricothyroid membrane with ultrasonography |
|
|
Thursday, 27 November 2025, Auditorium 93
09.15 - 09.55 Coffee, croissants and registration
10.00 - 10.15 Welcome and introduction: Airway management: what it is – and why should it be important?
Michael Seltz Kristensen, Camilla Strøm, Rasmus Hesselfeldt
10.15 - 10.40 Airway guidelines in action including the newest updates from DAS
Imran Ahmad
10.40 - 10.50 High flow nasal oxygenation
Zofia Piozik
10.50 - 11.05 BREAK
11.05 - 11.20 Rapid sequence induction
Imran Ahmad
11.20 - 11.30 Muscle relaxants
Matias Vested
11.35 - 11.55 Personalized videolaryngoscopy – an emerging concept
Martin Petzoldt
11.55 - 12.10 BREAK
12.10 - 12.30 Flexible scope intubation
Thomas Bøllingtoft Knudsen
12.30 - 12.45 Securing the airway awake and how to make it a pleasant experience
Jeppe Thue Jensen
12.45 - 12.55 Advanced airway management with simple equipment
Jeppe Thue Jensen, Rasmus Hesselfeldt
12.55 - 14.00 LUNCH at Restaurant Panza, Blegdamsvej 70
14.00 - 14.20 Advanced airway management by combining techniques
Camilla Strøm, Rasmus Hesselfeldt
14.20 - 14.45 Front of neck airway access
Rasmus Winkel and Jacob Melchiors
14.45 – 15:00 Extrathoracic, “cuirass”, ventilation
Jakob Friis Schmidt
15:00 - 15.15 BREAK
15.15 - 15.50 Paediatric airway management
Morten Bøttger
15.50 - 16.00 Ultrasonographic Identification of the airway in the neck
Robin Lin Lohse
After a little walk: Workshop, at the ENT-outpatient clinic, Entrance 7, 4th and 5th floor, section 7046/7056
16.15 - 16.30 Introduction to the workshop (4th floor section 7046, meeting room)
16.30 - 20.40 Hands-on workshop in small group rotations
All lecturers participate
20.40 - 23.00 After a refreshing 15 minute walk to the splendid restaurant BÆST, Guldbergsgade 29, 2200 København, we will continue the discussion of our cases while we enjoy a delightful dinner. We will end the day at the restaurant from where you can walk to central Copenhagen.
Friday, 28 November 2025, Auditorium 93
08.40 - 09.00 Coffee, espresso and croissants are served
09.00 - 10.15 Our own airway cases - What can we all learn?
Michael Seltz Kristensen, Michael Friis Tvede, Rasmus Hesselfeldt,
Camilla Strøm, Imran Ahmad, Martin Petzholdt and ALL
10.15 - 10.35 BREAK
10.35 - 10.55 Airway classification in the era of digitalization
Martin Petzoldt
10.55 - 11.15 The physiologically difficult airway and peri-oxygenation
Søren Steemann Rudolph
11.15 - 11.35 BREAK
11.35 - 11.55 From crisis to control – human factors, cognitive load and training
Imran Ahmad
11.55 - 12.20 Managing the bloody bleeding airway
Søren Steemann Rudolph
12.20 - 13.30 LUNCH at Panza
13.30 - 14.30 Our own Airway cases - What can we all learn?
Michael Seltz Kristensen, Michael Friis Tvede, Rasmus Hesselfeldt,
Camilla Strøm, Imran Ahmad, Martin Petzholdt and ALL
14.30 - 14.45 BREAK
14.45 - 15.05 Airway management in the neuro-/-traumatised. What’s different?
Karen-Lise Welling
15.05 - 15.20 ECMO – for emergency airway management
Karin Birgitta Egnell
15.20 - 15.40 Prehospital airway pitfalls
Dan Lou Isbye
15.40 - 16.00 Summary and diploma
Faculty, Michael Seltz Kristensen, Rasmus Hesselfeldt, Camilla Strøm
Airwaymanagement.dk is the online home of section for ENT-, Head-, Neck- and Maxillofacial Surgery at Department of Anaesthesia of Centre of Head and Orthopaedics at Rigshospitalet, University Hospital of Copenhagen, Denmark and our international partners.
We are an active working place with a production of more than 4.500 anaethesia's per year within the specialities of ENT and Head-, Neck- and Maxillofacial surgery.
Our flagship activity is Airway Management for Anaesthesiologists, an international, annual two-day airway course with a very extensive workshop and excellent ratings.
We try to be academically active, to constantly challenge our methods and to focus on post-graduate and post-specialist education.